The One Visit Crown (OVC) appears to be an increasingly popular and viable option to restore posterior teeth, such as those that are heavily broken down, heavily restored, exhibit cracked tooth syndrome (CTS), as well as restoration of endodontically treated teeth. However, one aspect that has been seldom discussed until now is use of the One Visit Crown where a high aesthetic is required.
The following case study of a notably discoloured maxillary first premolar highlights the ability to achieve a highly aesthetic result with placement of a One Visit Crown using a direct technique, which traditionally can appear challenging.
One Visit Crown (OVC) Clinical Case Study – Discoloured Maxillary Premolar
Figures 1 & 2 show a notably discoloured upper right first premolar tooth with an extensive amalgam filling on the disto-occlusal aspect.
 |
 |
| Figure 1 | Figure 2 |
The patient presented enquiring about options to cosmetically enhance this particular tooth, as she considered the appearance to now be socially unacceptable. After clinical and radiological examination, the tooth tested vital with no indication of pulpal necrosis or peri-apical pathology. A visible crack line was also noted on the mesial-marginal ridge (Figure 3).
 |
| Figure 3 |
Four treatment options were discussed with the patient:
- No treatment (not recommended)
- A large composite overlay restoration
- A traditional ceramic crown
- A One Visit Crown (OVC)
The One Visit Crown was chosen for financial reasons. The One Visit Crown can present a highly appealing treatment alternative to a traditional crown, as it can usually be completed by the clinician in a single visit, on average taking the clinician less than an hour and at a lesser fee.
In this particular case, a dark discoloured tooth creates a more challenging clinical scenario and therefore is potentially more difficult to achieve a good aesthetic result. This was conveyed to the patient prior, who understood the potential limitations of the treatment outcome.
The black case of each OVC contains an orange Occlusal Reduction Guide that helps determine sufficient occlusal reduction from tooth preparation, as well as McDonald Matrix Bands that are specific to the size of the OVC. The crown is in the lid under a light protected cover. Also included are two green OVC Wedges that are great for build ups such as in the case of deep marginal elevation (DME).
The tooth was isolated with rubber dam (Figure 5).
 |
|
| Figure 5 |
When significant tooth structure remains, rather than a traditional crown preparation with circumferential reduction of the tooth, the OVC procedure recommends minimal reduction in order to prepare the tooth for an adhesive onlay type restoration.
Minimal tooth preparation when preparing for aesthetic restorations has not only been shown to be better for the pulp1, but the compression dome concept after preparing a tooth in such a manner has also been shown to provide a strong coronal structure by forming a “stable peripheral bond in conjunction with a compressive design”2.
Once reduction was achieved (Figure 7), a slightly longer buccal bevel down to the gingival margin was created (Figure 8), in order to achieve a better shade blend to the discoloured tooth,
as well as provide more restorative space buccally in order to mask the discolouration.
 |
 |
| Figure 7 | Figure 8 |
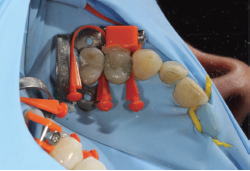
Figure 9 shows the McDonald Matrix Band and Stretch Wedges placed. Figure 10 shows the OVC in situ, with the majority of excess uncured material already removed.
 |
 |
| Figure 9 | Figure 10 |
Once the OVC was cured, the matrix band and wedges were removed. A greater buccal aesthetic was achieved by utilising the excess uncured OVC material on the buccal aspect of the tooth, along with flowable resin composite to restore along the gingival margin. The buccal material was then cured, and the restoration finished and polished to give the final aesthetic result (Figures 11 & 12).
 |
 |
| Figure 11 | Figure 12 |
In summary, the One Visit Crown offers a great treatment option to restore heavily-filled or broken-down posterior teeth.
These teeth can often be in an aesthetic zone, or patients may have a high aesthetic demand. In these situations, slight modifications to the traditional OVC technique can be utilised to achieve a greater aesthetic outcome. Both the cured, and uncured hybrid material are able to provide the clinician with a predictable aesthetic result, even when attempting to mask notable discolouration as shown in this clinical case study.
With a conservative preparation used wherever possible, the One Visit Crown can offer the clinician both a healthy and strong, yet aesthetic restorative solution for posterior teeth where indicated.
About Dr Sam Koh
 Dr Sam Koh is a Melbourne-based dentist, graduating from The University of Melbourne with First Class Honours. As the principal dentist of Orions Dental Taylors Lakes, his special interests are in Cosmetic Dentistry and Orthodontics.
Dr Sam Koh is a Melbourne-based dentist, graduating from The University of Melbourne with First Class Honours. As the principal dentist of Orions Dental Taylors Lakes, his special interests are in Cosmetic Dentistry and Orthodontics.
Dr Koh has been awarded with a prestigious fellowship from the International Academy of DentoFacial Esthetics in New York, as well as a fellowship in orthodontics. He is the co-founder of the Young Dentist Hub, and a KOL for the One Visit Crown as well as several other dental companies.
References
1. Ruiz, J. L. (2017) Supra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic Restorations. New York, New York:Wiley-Blackwell.
2. Milicich, G. (2017) The Compression Dome Concept – The Restorative Implications. Gen Dent. 65(5), 55-60.